


Former Drug Control Officials Lobby DEA Administrator Milgram
Guess who ghostwrote the letter

Yesterday, Marijuana Moment reported that “[s]ix former [DEA] heads and five former White House drug czars have sent a letter to the attorney general and current DEA administrator, voicing opposition to the top federal health agency’s recommendation to reschedule marijuana.”
To begin, recall that these former officials vociferously objecting to a Schedule III recommendation they likely haven’t seen, because the recommendation is not public. Hence, this lawsuit by me.
Upon learning of the letter, the main question I had is who wrote it. SAM (Smart Approaches for Marijuana), of course, posted the letter per the Marijuana Moment article. But, based on my quick social media review, they didn’t seem to publicly claim credit for writing it. Why not? It plainly did.
One thing you learn as a litigator is to inspect metadata.

Who is Jordan Davidson?
He works at SAM. So, yes, SAM—the non-profit spearheaded by Kevin Sabet—drafted the lobbying letter.
That should surprise nobody. After all, in March 2023, Sabet penned an essay with Senator James Lankford entitled “More Marijuana is Bad for Oklahoma.” Six months later, Senator Lankford sent a lobby letter to the DEA Administrator that links back to the Sabet/Lankford essay.
Who do you think the Lankford lobby letter?

And, if one follows Sabet or SAM’s rhetoric, it isn’t hard to recognize the talking points such as “[t]he FDA has not approved marijuana for medical use because no double-blind, published studies show safety and efficacy for raw marijuana; thus, it must remain a Schedule I drug.” That a drug must remain in Schedule I because a substance hasn’t been approved by the FDA is a proposition that the First Circuit Court of Appeals refuted. We have as well. The fact that six past DEA Administrators signed onto a statement repeating this canard illustrates precisely why every prior petition to reschedule marijuana has been denied.
The most recent lobbying letter also repeats the claim that “[r]esearch has found that 3 in 10 people who use marijuana become addicted to the drug”—a point that I believe Sabet didn’t candidly communicate in prior testimony.

The study continues to be presented in a misleading manner. For starters, the lobbying letter doesn’t link to the research, but the CDC website, which then cites the study entitled “Prevalence of Marijuana Use Disorders in the United States Between 2001–2002 and 2012–2013.” That adds a small layer of opacity.
I will link you to the paper. Its conclusion? “While not all marijuana users experience problems, nearly 3 of 10 marijuana users manifested a [DSM IV] marijuana use disorder in 2012–2013.” To be clear, this is a statistic of among marijuana users. The overall “prevalence of DSM-IV marijuana use disorder was 1.5% (0.08) in 2001–2002 and 2.9% (SE, 0.13) in 2012–2013 (P < .05).”
That’s not nothing. But of course, consider that unlike other addictions (e.g., alcohol), a pot addiction won’t kill. It may turn you into a couch potato.

This is important. Head counts don’t reflect magnitude of societal harm. I’m no doctor, but it seems evident that a benzo addiction is far worse than a bud addiction. Why hasn’t Smart Approaches to Coffee (SAC) touted studies showing that 30% of caffeine users in Vermont meet the DSM-IV criteria for caffeine use disorder or the fact that “[p]revalence estimates for CUD currently lie between 6% and 13.9%.” Caffeine? Not so dangerous. The prevalence of marijuana use disorder—whether among cannabis users or more generally—just doesn’t provide the complete picture.
How the “3” in the 3 in 10 is counted: Past-year marijuana use and DSM-IV marijuana use disorder (abuse or dependence). This is important too. Per a different paper:
DSM-IV requires that three of the six criteria be met for a diagnosis of cannabis dependence, and that one of the four criteria be met for a diagnosis of cannabis abuse (American Psychiatric Association, 1994). Therefore, a wide variety of symptom combinations could qualify for the diagnoses of substance abuse or dependence, but the actual heterogeneity that exists in cannabis use disorders is unknown.
Those criteria are:
(1) development of tolerance; (2) using cannabis in larger amounts or over a longer period than intended; (3) inability to cut down or reduce cannabis use; (4) spending large amounts of time to obtain, use, or recover from the effects of cannabis; (5) giving up important social, occupational, or recreational activities in favor of using cannabis; (6) continued use of cannabis despite its adverse consequences.
I’ll let you judge for yourself whether meeting 3 out of 6 criteria above is cause for concern. My greater concern is the notion that 3 out of 10 users “become addicted” to marijuana. The suggestion is that 3 out of 10 that smokes a joint will become addicted. But that’s not rights. Of those that use marijuana, 3 out of 10 have a dependence or use disorder. A subtle but important difference.
Also note that the “prevalence of past-year DSM-IV marijuana use disorder among users was 35.6% in 2001–2002 and 30.6% in 2012–2013.” So, as state laws increasingly tolerated marijuana use, marijuana use disorder remained the same or went down. This conclusion is explicit in the paper: “while Δ-9-THC potency in marijuana continued to increase from 2001–2002 to 2012–2013, the risk for marijuana use disorder among users decreased.”1
Whatever you may think about the folks drafting and signing these letters, and the interests they represent—they are not incompetent. Actually, SAM is extremely competent with a relatively lean budget that focuses on spending money on canvassing important people as opposed to late-fall bacchanals.
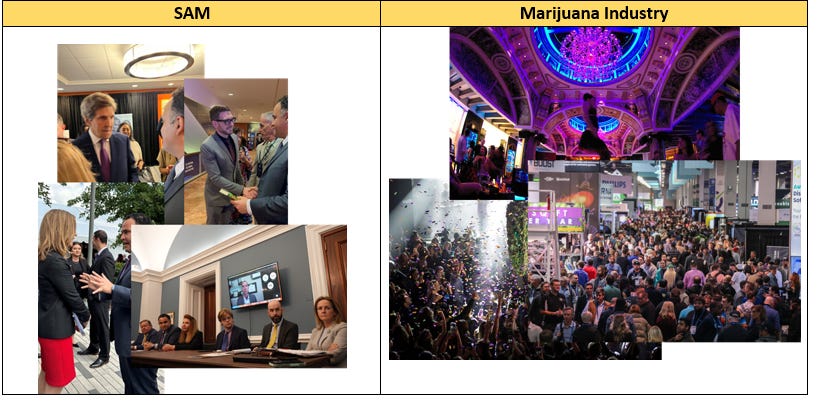
They are effective too. On this, they have my respect. For example, what is the only legislative reform regarding marijuana to have ever gotten through Congress? Return to Davidson’s bio above: “Shepherd[ed]” by SAM.
As Shane repeatedly warned, the Medical Marijuana and Cannabidiol Research Expansion Act in fact makes marijuana research harder not easier. And yet, it received wide, bipartisan phrase.
Let me give you my read of all this. SAM wants Schedule I. Realistically, however, it knows Schedule I can’t politically happen. But, it can set goal posts there. And, it can hope that the current Administrator will listen to past senior drug policy officials. Maybe, she splits the difference between Schedule I and the coveted Schedule III. Certainly, this letter and the others provide some cover.2
Ordinarily, the idea that DEA would land on a higher schedule than HHS would be a very bad legal bet. Still, I wouldn’t bet on it here. But because of the treaty issue, it is a real legal possibility. Also, these letters may constitute “other relevant data” the Administrator can consider before proposing a schedule, above and beyond the HHS recommendation/evaluation.
Consider this too. Although the DEA Administrator suggested that DEA will first propose a rule and then open up a comment period before landing on a final rule, the fact is that, like people, comments rarely dislodge an agency’s initial position. The agency makes its mind up before proposing the rule, not after. So, the best time to communicate positions to DEA may be now, before the agency proposes the rule.
Finally, consider this late paragraph of the SAM lobbying letter:
Moving marijuana to Schedule III would supersize the cannabis industry in the United States by allowing them to evade IRS Section 280E and deduct business expenses. Not only would this mean that marijuana corporations would be able to deduct expenses for advertisements appealing to youth and the sale of kid-friendly marijuana gummies, but it would also dramatically increase the industry’s commercialization ability.
Never mind the difference between “evad[ing]” 280E and rendering it inapplicable. The more important observation is the suggestion. So long as DEA doesn’t move marijuana to schedule III the cannabis industry won’t be “supersize[d].” The compromise solution is thus implicitly suggested: Schedule II. Or, better yet, staggered rescheduling. SAM et al. would be elated with either outcome, which allow some political face saving while denying the cannabis industry all benefits of rescheduling.
Conclusion
Ultimately, I agree with Kyle Jaeger’s take. The letter and SAM spamming the DEA isn’t some earth-shattering development. But it is also not nothing.
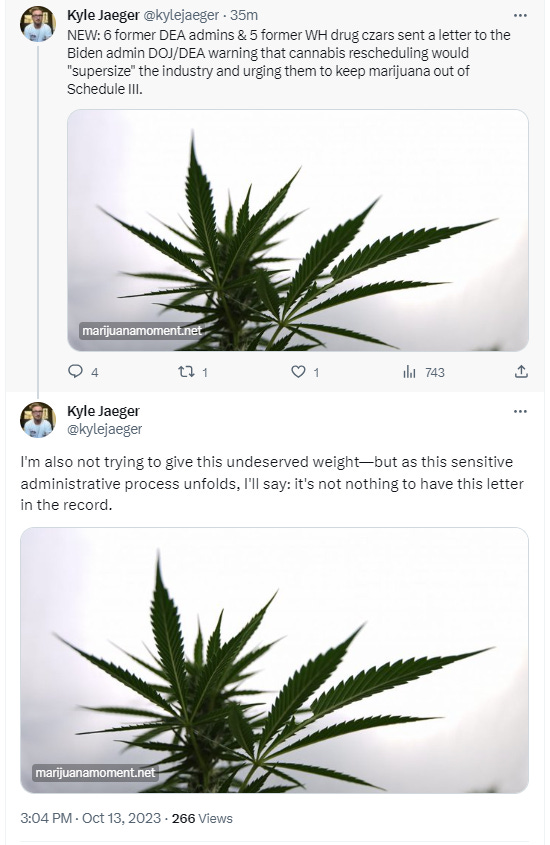
More important, the letter shows us that the prohibitionist side has mobilized, organized, and activated now that the process has shifted to its home turf at DEA. Will the cannabis movement counter this in this existential moment?
Postscript
Kevin, I accept. I’ll debate you—just on the merits.3 Maybe Nick Gillespie can moderate.
It is also unclear to me whether the study distinguishes between medical and non-medical use. One can become addicted to a substance (i.e., develop a use disorder) even though the substance is being used medicinally.
These letters are going to the Administrator as opposed to the President or anyone else. That is to whom any similar letters ought to be addressed at this juncture of the administrative process.
Also, I don’t think you are a “weak little cupcake”; you make good points, on the merits, and there is a lot of common ground.
great post!
Hey maybe file FOIA on research and data from the "Cancer" research done at Fort Detrick, MD...that started in the late 70's early 80's to present. I'd love to see their response as well as the data. It's crazy but the strains they produced are still obtainable in the industry today. Like G13... Just saying